Читайте также:
|
Communication
Blood is a connective tissue. It provides one of the means of communication between the cells of different parts of the body and the external environment, e.g. it carries:
• oxygen from the lungs to the tissues, and carbon dioxide from the tissues to the lungs for excretion
• nutrients from the alimentary tract to the tissues, and cell wastes to the excretory organs, principally the kidneys
• hormones secreted by endocrine glands to their target glands and tissues
• heat produced in active tissues to other less active tissues
• protective substances, e.g. antibodies, to areas of infection
• clotting factors that coagulate blood, minimizing bleeding from ruptured blood vessels.
Blood makes up about 7% of body weight (about 5.6 litres in a 70 kg man). This proportion is less in women and considerably greater in children, gradually decreasing until the adult level is reached.
Blood in the blood vessels is always in motion because of the pumping action of the heart. The continual flow maintains a fairly constant environment for the body cells.
Blood volume and the concentration of its many constituents are kept within narrow limits by homeostatic mechanisms.'
Blood is composed of a straw-coloured transparent fluid, plasma, in which different types of cells are suspended. Plasma constitutes about 55% and cells about 45% of blood volume (Fig. 4.1 A).
PLASMA
The constituents of plasma are water (90 to 92%) and dissolved substances, including:
• plasma proteins
• inorganic salts
• nutrients, principally from digested foods
• waste materials
• hormones
• gases.
Plasma proteins
Plasma proteins, which make up about 7% of plasma, are normally retained within the blood, because they are too big to escape through the capillary pores into the tissues. They are largely responsible for creating the osmotic pressure of blood (normally 25 mmHg or 3.3 kPa), which keeps plasma fluid within the circulation. If plasma protein levels fall, because of either reduced production or loss from the blood vessels, osmotic pressure is also reduced, and fluid moves into the tissues (oedema) and body cavities.
Plasma viscosity (thickness) is due to plasma proteins, mainly albumin and fibrinogen. Viscosity is used as a measure of the body's response to some diseases.
Albumins. These are formed in the liver. They are the most abundant plasma proteins and their main function is to maintain normal plasma osmotic pressure. Albumins also act as carrier molecules for lipids and steroid hormones. -
Globulins. Most are formed in the liver and the remainder in lymphoid tissue. Their main functions are:
• as antibodies (immunoglobulin), which are complex proteins produced by lymphocytes that play an important part in immunity. They bind to, and neutralise, foreign materials (antigens) such as microorganisms (see also p. 376).
• transportation of some hormones and mineral salts; e.g. thyroglobulin carries the hormone thyroxine and transferrin carries the mineral iron
• inhibition of some proteolytic enzymes, e.g. a2 macroglobulin inhibits trypsin activity.
Clotting factors. These are substances essential for coagulation of blood (p. 66). Serum is plasma from which clotting factors have been removed (Fig. 4.IB).
Fibrinogen. This is synthesised in the liver and is essential for blood coagulation.
Inorganic (mineral) salts
These are involved in a wide variety of activities, including muscle contraction, transmission of nerve impulses, formation of secretions and maintenance of acid-base balance. In health the blood is slightly alkaline. Alkalinity and acidity are expressed in terms of pH, which is a measure of hydrogen ion concentration, or [H+] (p. 21 and Fig. 2.6). The pH of blood is maintained between 7.35 and 7.45 by an ongoing complicated series of chemical activities, involving buffering systems.
Nutrients
In the alimentary tract, food is broken down into small molecules, e.g. monosaccharides, amino acids, fatty acids and glycerol, and are absorbed. Together with mineral salts they are required by all body cells to provide energy, heat, materials for repair and replacement, and for the synthesis of other blood components and body secretions.
Waste products
Urea, creatinine and uric acid are the waste products of protein metabolism. They are formed in the liver and conveyed in blood to the kidneys for excretion.
Hormones
These are substances synthesised by endocrine glands. Hormones pass directly from the endocrine cells into the blood, which transports them to their target tissues and organs elsewhere in the body, where they influence cellular activity.
Gases
Oxygen, carbon dioxide and nitrogen are transported round the body dissolved in plasma. Oxygen and carbon dioxide are also transported in combination with haemoglobin in red blood cells (p. 60). Most oxygen is
carried in combination with haemoglobin and most carbon dioxide as bicarbonate ions dissolved in plasma. Atmospheric nitrogen enters the body in the same way as other gases and is present in plasma but it has no physiological function.
CELLULAR CONTENT OF BLOOD
There are three types of blood cells (see Fig. 1.5, p. 8).
• erythrocytes (red cells)
• platelets (thrombocytes)
• leukocytes (white cells).
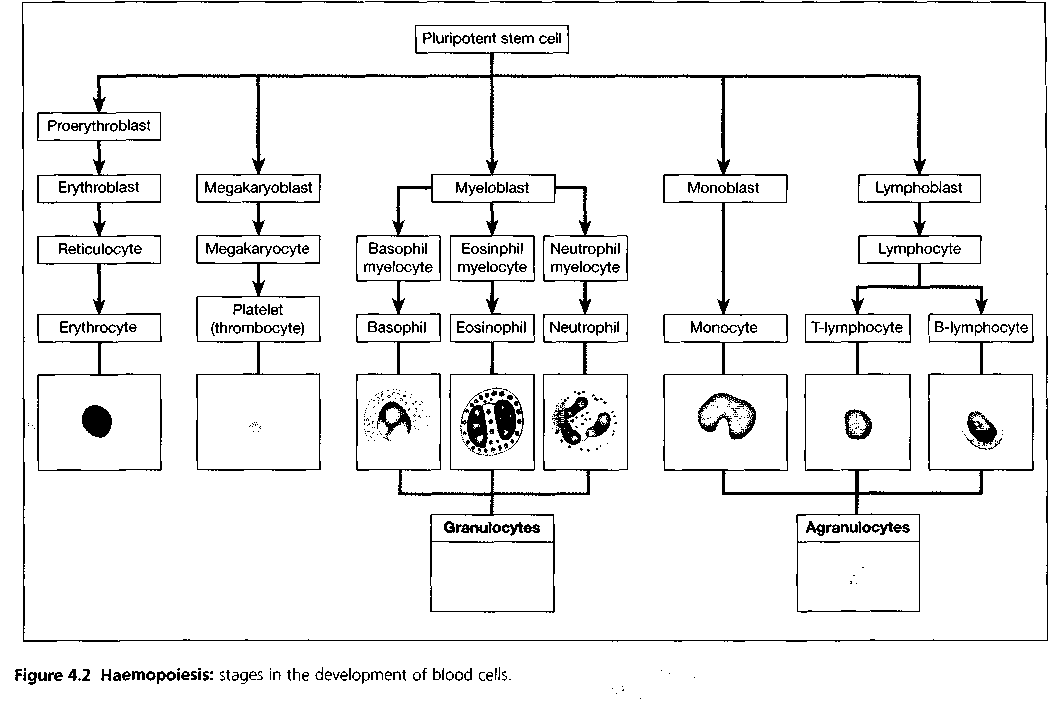
All blood cells originate from pluripotent stem cells and go through several developmental stages before entering the blood. Different types of blood cells follow separate lines of development. The process of blood cell formation is called haemopoiesis (Fig. 4.2) and takes place within red bone marrow. For the first few years of life, red marrow occupies the entire bone capacity and, over the next 20 years, is gradually replaced by fatty yellow marrow that has no haemopoietic function. In adults, haemopoiesis in the skeleton is confined to flat bones, irregular bones and the ends (epiphyses) of long bones, the main sites being the sternum, ribs, pelvis and skull. In addition, some lymphocytes (white blood cells) are produced in lymphoid tissue.
Erythrocytes (red blood cells)
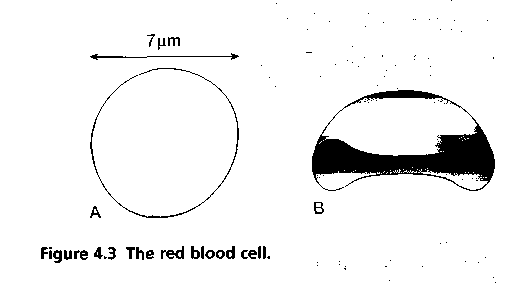
Red blood cells are biconcave discs; they have no nucleus, and their diameter is about 7 micrometres (Fig. 4.3). Their main function is in gas transport, mainly of oxygen, but they also carry some carbon dioxide. Their characteristic shape is suited to their purpose; the biconcavity increases their surface area for gas exchange, and the thinness of the central portion allows fast entry and exit of gases. The cells are flexible so they can squeeze through narrow capillaries, and contain no intracellular organelles, leaving more room for haemoglobin, the large pigmented protein responsible for gas transport.
Measurements of red cell numbers, volume and haemoglobin content are routine and useful assessments made in clinical practice (Table 4.1). The symbols in brackets are the abbreviations commonly used in laboratory reports.
Life span and function of erythrocytes
Erythrocytes are produced in red bone marrow, which is present in the ends of long bones and in flat and irregular
bones. They pass through several stages of development before entering the blood. Their life span in the circulation is about 120 days.
The process of development of red blood cells from pluripotent stem cells takes about 7 days and is called erythropoiesis (Fig. 4.2). The immature cells are released into the bloodstream as reticulocytes, and then mature into erythrocytes over a day or two within the circulation. During this time, they lose their nucleus and therefore become incapable of division (Fig. 4.4).
 Both vitamin B12 and folic acid are required for red blood cell synthesis. They are absorbed in the intestines, although vitamin B12 must be bound to intrinsic factor (p. 295) to allow absorption to take place. Both vitamins are present in dairy products, meat and green vegetables. The liver usually contains substantial stores of vitamin B]2, several years' worth, but signs of folic acid deficiency appear within a few months.
Both vitamin B12 and folic acid are required for red blood cell synthesis. They are absorbed in the intestines, although vitamin B12 must be bound to intrinsic factor (p. 295) to allow absorption to take place. Both vitamins are present in dairy products, meat and green vegetables. The liver usually contains substantial stores of vitamin B]2, several years' worth, but signs of folic acid deficiency appear within a few months.
LEUKOCYTES (WHITE BLOOD CELLS)
These cells have an important function in defending the body against microbes and other foreign materials. Leukocytes are the largest blood cells and they account for about 1% of the blood volume. They contain nuclei and some have granules in their cytoplasm. There are two main types (Table 4.2):
• granulocytes (polymorphonuclear leukocytes)
- neutrophils, eosinophils and basophils
• agranulocytes
- monocytes and lymphocytes.
Granulocytes (polymorphonuclear leukocytes)
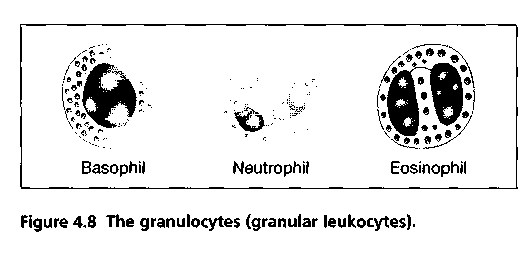
During their formation, granulopoiesis, they follow a common line of development through myeloblast to myelocyte before differentiating into the three types (Figs 4.2 and 4.8). All granulocytes have multilobed nuclei in their cytoplasm. Their names represent the dyes they take up when stained in the laboratory. Eosinophils take up the red acid dye, eosin; basophils take up alkaline methylene blue; and neutrophils are purple because they take up both dyes.
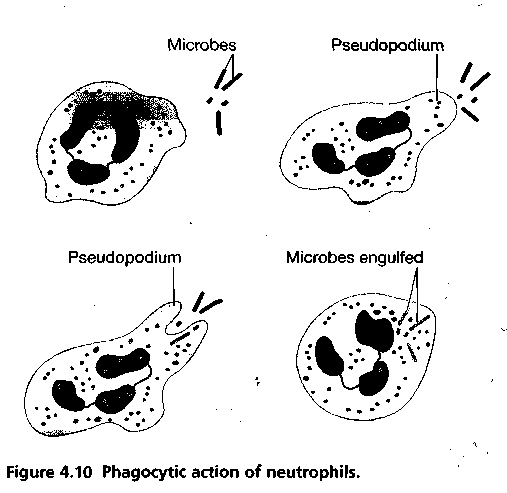
Neutrophils
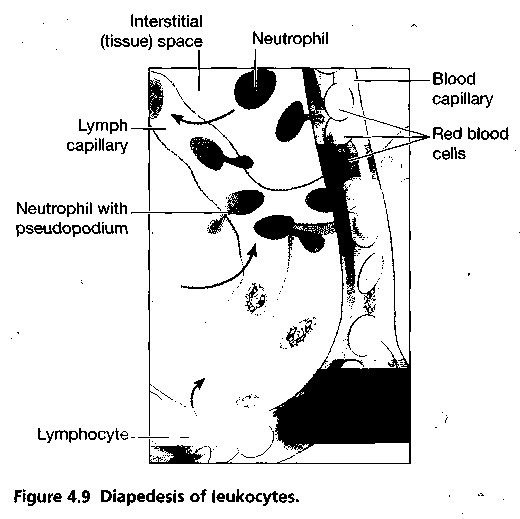
 Their main function is to protect against any foreign material entering the body, mainly microbes, and to remove waste materials, e.g. cell debris. They are attracted in large numbers to any area of infection by chemical substances, released by damaged cells, called chemotaxins. Neutrophils are highly mobile, and squeeze through the capillary walls in the affected area by diapedesis (Fig. 4.9). Thereafter they engulf and kill the microbes by phagocytosis (Fig. 4.10). Their nuclei are characteristically complex, with up to six lobes, and their granules are lysosomes containing enzymes to digest engulfed material. Pus that may form in an infected area consists of dead tissue cells, dead and live microbes, and phagocytes killed by microbes.
Their main function is to protect against any foreign material entering the body, mainly microbes, and to remove waste materials, e.g. cell debris. They are attracted in large numbers to any area of infection by chemical substances, released by damaged cells, called chemotaxins. Neutrophils are highly mobile, and squeeze through the capillary walls in the affected area by diapedesis (Fig. 4.9). Thereafter they engulf and kill the microbes by phagocytosis (Fig. 4.10). Their nuclei are characteristically complex, with up to six lobes, and their granules are lysosomes containing enzymes to digest engulfed material. Pus that may form in an infected area consists of dead tissue cells, dead and live microbes, and phagocytes killed by microbes.
There is a physiological increase in circulating neutrophils following strenuous exercise and in the later stages of normal pregnancy. Numbers are also increased in:
• microbial infection
• extensive tissue damage, e.g. inflammation, myocardial infarction, burns, crush injuries
• metabolic disorders, e.g. diabetic ketoacidosis, acute gout
• leukaemia
• heavy smoking
• use of oral contraceptives.
Eosinophils
Eosinophils, although capable of phagocytosis, are less active in this than neutrophils; their specialised role appears to be in the elimination of parasites, such as worms, which are too big to be phagocytosis. They are equipped with certain toxic chemicals, stored in their granules, which they release when the eosinophil binds an infecting organism.
Eosinophils are often found at sites of allergic inflammation, such as the asthmatic airway and skin allergies. There, they promote tissue inflammation by releasing their array of toxic chemicals, but they may also dampen down the inflammatory process through the release of other chemicals, such as an enzyme that breaks down histamine (p. 372).
Basophils
Basophils, which are closely associated with allergic reactions, contain cytoplasmic granules packed with heparin (an anticoagulant), histamine (an inflammatory agent) and other substances that promote inflammation. Usually the stimulus that causes basophils to release the contents of their granules is an allergen (an antigen that causes allergy) of some type. This binds to antibody-type receptors on the basophil membrane. A cell type very similar to basophils, except that it is found in the tissues, not in the circulation, is the mast cell. Mast cells release their granule contents within seconds of binding an allergen, which accounts for the rapid onset of allergic symptoms following exposure to, for example, pollen in hay fever (p. 379).
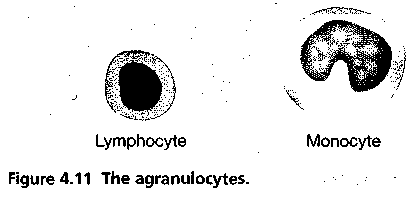
Agranulocytes
The types of leukocyte with a large nucleus and no granules in their cytoplasm are monocytes and lymphocytes and they make up 25% to 50% of all leukocytes (Figs 4.2 and 4.11).
Monocytes
These are large mononuclear cells that originate in red bone marrow. Some circulate in the blood and are actively motile and phagocytic while others migrate into the tissues where they develop into macrophages.^ Both types of cell produce interleukin 1, which:
• acts on the hypothalamus, causing the rise in body temperature associated with microbial infections
• stimulates the production of some globulins by the liver
• enhances the production of activated T-lymphocytes.
Macrophages have important functions in inflammation (p. 371) and immunity.
The monocyte-macrophage system. This is sometimes called the reticuloendothelial system, and consists of the body's complement of monocytes and macrophages. Some macrophages are mobile, whereas others are fixed. Collections of fixed macrophages include:
• histiocytes in connective tissues
• synovial cells in joints
• Langerhans cells in the skin
• microglia in the brain
• Kupffer cells in the liver
• alveolar macrophages in the lungs
• sinus-lining macrophages (reticular cells) in the spleen, lymph nodes and thymus gland
• mesangial cells in the glomerulus of nephrons in the kidney
• osteoclasts in bone.
Macrophages have a diverse range of protective functions. They are actively phagocytic and if they encounter large amounts of foreign or waste material, they tend to multiply at the site and 'wall off the area, isolating the material, e.g. pockets of tubercular infection in the lungs. They synthesise and release an array of biologically active chemicals, called cytokines, including interleukin 1 mentioned earlier. They also have a central role linking the non-specific and specific (immune) systems of body defence (Ch. 15), and produce factors important in inflammation and repair.
Their numbers are increased in microbial infections, collagen diseases and some non-infective bowel conditions.
Lymphocytes
Lymphocytes are smaller than monocytes and have large nuclei. They circulate in the blood and are present in great numbers in lymphatic tissue such as lymph nodes and the spleen. Lymphocytes develop from pluripotent stem cells in red bone marrow and from precursors in lymphoid tissue, then travel in the blood to lymphoid tissue elsewhere in the body where they are activated, i.e. they become immunocompetent which means they are able to respond to antigens (foreign material). Examples of antigens include:
• cells regarded by lymphocytes as abnormal, e.g. cells that have been invaded by viruses, cancer cells, tissue transplant cells
• pollen from flowers and plants
• fungi
• bacteria
• some large molecule drugs, e.g. penicillin, aspirin.
Although all lymphocytes originate from one type of stem cell, when they are activated in lymphatic tissue, two distinct types of lymphocyte are produced -
T-lymphocytes and B-lymphocytes. The specific functions of these two cell types are discussed in Chapter 15.
PLATELETS (THROMBOCYTES)
These are very small non-nucleated discs, 2 to 4 μm in diameter, derived from the cytoplasm of megakaryocytes in red bone marrow (Fig. 4.2). They contain a variety of substances that promote blood clotting, which causes haemostasis (cessation of bleeding).
The normal blood platelet count is between 200 × 109/1 and 350 × 109/1 (200 000 to 350 000/mm3). The control of platelet production is not yet entirely clear but one stimulus is a fall in platelet count. The kidneys release a substance called thrombopoietin, which stimulates platelet synthesis; other cytokines may also be involved.
The lifespan of platelets is between 8 and 11 days and those not used in haemostasis are destroyed by macrophages, mainly in the spleen. About a third of platelets are stored within the spleen rather than in the circulation; this is an emergency store that can be released as required to control excessive bleeding.
Дата добавления: 0000-00-00; просмотров: 170 | Нарушение авторских прав
| <== предыдущая страница | | | следующая страница ==> |
| и глаголом to be или любым другим глаголом во 2 лице, мн. числе | | | Программа развития деятельности студенческих объединений 2014 |