
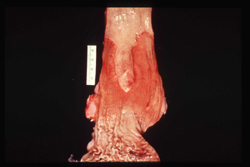
| 49. Prostate gland: prostatic hyperplasia The prostate gland has an outer rim (peripheral zone), central zone, and transitional zone, the latter surrounding the prostatic urethra. The gland is under the control of dihydrotestosterone (DHT). Recall that DHT is normally responsible for development of the prostate in the fetus, hence an increase in DHT leads to benign prostatic hyperplasia (BPH). BPH primarily occurs in the transitional zone around the urethra. Note how the prostate gland literally bulges (see arrow) when sectioned. Nodular areas are noted throughout the gland and represent areas of hyperplasia. The surrounding hyperplastic tissue compresses the prostatic urethra in the center of the gland. Symptoms of BPH relate to urethral obstruction. Symptoms include delayed initiation of the urinary stream, narrow urinary stream, increased frequency of urination (patient often wakes up at night to urinate), dribbling at the end of urination, and the possibility of complete obstruction to urine flow. Complete obstruction of urinary flow causes a back-up of urine into the bladder. This backup of urine dilates the bladder and causes hypertrophy of the smooth muscles in the bladder wall, since they are contracting against increased resistance.Furthermore, the urine backs up into the ureters (dilated) and renal pelvises causing dilatation. This is called hydronephrosis. | |
Cell Injury
Post 5: (Dated: Jan 16 - 2009)
Gravid uterus (after delivery): 50% hypertrophy, 50% hyperplasia ---> of smooth muscles. Also Goiter in iodine deficiency!!

| 54. Uterus: gravid uterus Note the marked enlargement of the gravid uterus. This is secondary to an equal amount of both hyperplasia and hypertrophy of smooth muscle cells under the stimulation of estrogen. Recall that smooth muscle cells are stable cells, hence they may undergo both hypertrophy and hyperplasia. Striated muscle and cardiac muscle are permanent cells and are only capable of undergoing hypertrophy. (Ci053) |
Normal 3 times many WBC than RBC
RBC hyperplasia in BoneMarrow may be caused by COPD ---> hypoxemia ---> raised Epo
Erythropoetin is made in the endothelial cells of the peri-tubular capillaries

| 51. Bone marrow: RBC hyperplasia Normally, there should be a 3:1 ratio of leukocytes to RBCs. However, most of the nucleated cells in this smear are erythroid precursors, hence RBC hyperplasia is present. The stimulus, in most cases, is tissue hypoxia with release of erythropoietin(hormone) from the endothelial cells of the peritubular capillaries in the kidneys. If this smear was from a patient returning from a three-week trip in the Andes mountains, it would be an example of physiologic hyperplasia. However, if it was a smear from a smoker with COPD, it would be pathologic hyperplasia. (Ci225) |
Psoriasis: Silvery Scales is an unregulated proliferation of squamous cells in the skin (hyperplasia).
Treatment: MTX (works on the basal cells from proliferating).

| 52. Skin: psoriasis (pathologic hyperplasia)Note the raised, erythematous skin lesion covered by silvery scales. This is the classic appearance and location for psoriasis. It is due to an unregulated hyperplasia of squamous cell proliferation in the epidermis. (Ci226) | |

| 53. Skin: histologic section of psoriasis (pathologic hyperplasia) Note the increase in stratum corneum surfacing the epidermis. This corresponds to the silvery scales in the previous slide. Also note the increased overall thickness of the epidermis owing to hyperplasia. Recall that the cells in the basal cell layer are stem cells (labile cells). (Ci227) |
All hormone stimulated glands go through hyperplasia, not hypertrophy.
Urinary bladder goes through hypertrophy of smooth muscle cells related to afterload caused by urethra narrowing due prostate hyperplasia.

| 50. Prostate and bladder:prostatic hyperplasia with subsequent hypertrophy of the muscle in the bladder wall Normally, the prostate gland has an outer rim (peripheral zone), central zone, and transitional zone, the latter surrounding the prostatic urethra. The gland is under the control of dihydrotestosterone (DHT, recall that DHT is normally responsible for development of the prostate in the fetus), hence an increase in DHT leads to benign prostatic hyperplasia (BPH). BPH primarily occurs in the transitional zone around the urethra. Note how the cut surface of the prostate gland bulges (see arrow). Nodular areas are noted throughout the gland and represent areas of hyperplasia. The surrounding hyperplastic tissue compresses the prostatic urethra in the center of the gland. Symptoms of BPH relate to urethral obstruction. Symptoms include delayed initiation of the urinary stream, narrow urinary stream, increased frequency of urination (patient often wakes up at night to urinate), dribbling at the end of urination, and the possibility of complete obstruction to urine flow. Complete obstruction of urinary flow causes a back up of urine into the bladder. This backup of urine dilates the bladder and causes hypertrophy of the smooth muscles in the bladder wall, since they are contracting against increased resistance. Furthermore, the urine backs up into the ureters (dilated) and renal pelvises causing dilatation. This is called hydronephrosis. (Ci052) |
Gum hyperplasia in phenytoin therapy??
Metaplasia ---> replacement of one adult cell type by other!!
Vitamin A deficiency--> cornea --> cuboidal epi. --> squamous metaplasia!!
Vit A prevents sq. metaplasia!!
Barret’s esophagus(Metaplasia) = glandular cells, mucus secreting, goblets cells instead of squamous cell epi. ---> precursor of adenocarcinoma
| 55. Distal esophagus and proximal stomach: gastroesophageal reflux disease (GERD) with ulceration Subjacent to the ruler, note the extreme ulceration of the mucosal surface of the distal esophagus (reddened area) leaving only a midline tongue of residual esophageal mucosa. The ulceration is due to an incompetent lower esophageal sphincter and reflux of acid into the distal esophagus. Note the proximal stomach rugae at the bottom of the slide.(Ci228) | |
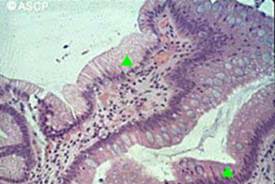
| 56. Distal esophagus: glandular metaplasia secondary to acid reflux (Barrett’s esophagus) The distal esophagus should be lined by squamous epithelium. However, due to acid reflux from the stomach into the distal esophagus (gastroesophageal reflux disease - GERD), the epithelium has undergone glandular metaplasia (called Barrett's esophagus) with mucin production as a reaction to acid injury. In GERD, the lower esophageal sphincter is relaxed which allows for acid reflux into the distal esophagus. The arrows point to glandular tissue synthesizing mucin (top arrow) and glandular tissue that has differentiated into goblet cells (bottom arrow). If left untreated with antacids (e.g., Mylanta) and drugs that prevent acid production (e.g., H2 blockers of parietal cell, proton blockers), glandular metaplasia may progress into glandular dysplasia and adenocarcinoma. Distal esophageal adenocarcinoma due to a Barrett's esophagus has now replaced squamous carcinoma of the esophagus as the most common primary esophageal cancer.( Ci054) | |
| 57. Distal esophagus: special stain enhancing the presence of glandular metaplasia secondary to acid reflux (Barrett�s esophagus) Note the red staining mucous and blue-staining mucin in the goblet cells. (Ci055) |
Lining of main stem bronchus --->cilliated psuedostratified columnar ---> in smoker ---> undergo sqaumous metaplasia!!
Increase Goblet cells in main stem bronchus ---> hyperplasia
smokers have goblet cells in terminal bronchioles ---> metaplasia (normally no goblet cells in this place)
If goblet cells in stomach = abnormal ---> should be present in s.intestine ---> glandular metaplasia ---> precursor for adenocarcinoma of stomach
H. Pylori is the most common cause of adenocarcinoma of the stomach ---> produce damage to the pylorus and antral mucosa ---> chronic atrophic gastritis with intestinal glandular metaplasia ---> precursor lesion for adenocarcinoma
Lung: Cilliated columnar epithelium ---> sqaumous metaplasia ---> dysplasia ---> Cancer Sq Carcinoma
Distal Esophagus: Sq ---> glandular epithelium, mucus secreting ---> defense against acid injury ---> may go into atypical metaplasia ---> adenocarcinoma
Two parasites can produce cancer:
Дата добавления: 2015-10-24; просмотров: 139 | Нарушение авторских прав
| <== предыдущая страница | | | следующая страница ==> |
| Vinca Alkaloids(vincristin, vinblastin) works on mitotic spindles(made from periwinkle plant); | | | I know some people that could help you. |