|
Читайте также: |
As outlined in Appendix Figure 1 Type Two Diabetes is more spread in rural areas, where communities are. So, again the information of type 2 diabetes prevalence among Aborigines is confirmed by location of this disease.
Chronic diseases such as diabetes and those related to it account for 59% of the difference in mortality between Indigenous and non-Indigenous Australians. One of the most important issues to be solved by health services is to prevent and manage risks of type 2 diabetes amongst Indigenous Australians (Snowdon, 2012).
Currently Indigenous people are in more dangerous situation because of too many cases of type 2 diabetes. This disease has major complications on Aboriginal people. The Aboriginal and Torres Strait Islander peoples have a much earlier age for onset of diabetes with the prevalence of diabetes in the 25-34 year age group in one central Australian community being 13% compared to 0.3% in the general Australian population (Shukla, 2010).
The death rate in Indigenous communities is believed to be up to 17 times higher than that of non-Indigenous Australians, mainly due to high levels of cardiovascular disease and kidney disease associated with diabetes. Complications include a higher risk of heart attack or stroke, eye disease, kidney disease and nerve damage, which may result in traumatic injury, infection and possible limb amputation (Snowdon, 2012). Statistics of complications and death incidents is alarming because the Indigenous population can be eradicated in a few decades or even less.
In Queensland, more than 200 pharmacies and health centres distribute NDSS products. As stated by the Queensland Government one can contact your local GP to organise screening tests. If one has type 2 diabetes, a range of professionals can help by managing your health over the longer term, including:
•your GP
•diabetes educators such as nurses, dieticians, podiatrists or pharmacists with a special interest in diabetes
•exercise professionals, such as a physiotherapist or a personal trainer
•optometrists and ophthalmologists
•counsellors and psychologists
•other professionals that can help meet your personal healthcare needs.
(Queensland Government, 2012)
There are numbers of organisations which provide help in preventing and managing type 2 diabetes among Aboriginals. Such an organisation is Aboriginal and Torres Strait Islander Program (A&TSI) developed many programs to support healthcare in communities and raise literacy rate amongst indigenes people.
3.2 Effect of Diabetes on Aboriginals/Communities
Due to often incidents of type 2 diabetes in communities many people began leaving their communities as a result of lack of health services. It is hard to get appropriate treatment from specialists, because communities are mainly located in rural areas under poor conditions far from big cities. Another reason is rural, poor conditions to live. This feature of these all communities has resulted in poor nutrition and type 2 diabetes.
Living in the communities is cultural part of Indigenous people. Decay of communities leads to loss of Indigenous traditions and language.
There is another important damaging effect of type 2 diabetes on Aboriginal people and their communities – disability to work, as a result of the complications cause by this disease. So, this issue causes poverty in families and communities.
Current Management Strategies
Medical Strategies
The Aboriginal and Torres Strait Islander Chronic Disease Fund is a consolidation of programs from the Indigenous Chronic Disease Package. Its objectives are to improve the prevention, detection and management of chronic disease in Aboriginal and Torres Strait Islander peoples to increase life expectancy. In Appendix Figure 2 a list of Australian Government contributions to manage chronic disease amongst Aboriginals is outlined. All the outcomes have positive influence on Indigenous population.
Queensland Health is developing a Chronic Disease Strategy for Indigenous people, mainly based on recommendations to improve health services. Systematic and coordinated primary health care is essential to improve the health of Indigenous Australians. Service providers organize funding of national diabetes/nutrition coordinator, support primary care services. A National Public Health Nutrition Strategy has rather influential impacts on managing type 2 diabetes disease among Aboriginals (Queensland Government, 2012).
Medical strategies such as hospitalisation, nursing and visiting doctors, etc., will have a positive contribution towards Aboriginals health. These strategies are expected to be improved by Government funding and local support. In rural areas health services can’t provide appropriate help, so, that is why Queensland Strategy is to provide special equipment, specialists and buildings (Queensland Strategy for Chronic Disease, 2005-2015).
Social Strategies
There are a lot of social programs which are providing strategies to manage type 2 Disease. Australian Diabetes organisation organise education, nutrition and exercise support to patients. But the most significant activity was implemented by Queensland Government, Queensland Strategy for Chronic Disease 2005-2015 report outlines all latest goals to improve the type 2 diabetes situation. Nutrition, housing and education strategies are as important as health service. Improved conditions of people’s life styles will be the best prevention from this chronic disease.
Proposed strategies to Manage Diabetes for Aboriginals
In Indigenous Australians, Type 2 Diabetes is not just a disease of poor diet and lack of exercise but rather is caused by risk factors acting together, which include low socioeconomic status and geographical isolation. It is important to understand these risk factors and the culture of the Aboriginal and Torres Strait Islander people before planning treatments, to allow for better outcomes and managements of the disease.
Two proposals are recommended to manage Type 2 Disease amongst Aboriginal and Torres Strait Islander people:
1. Increase the collaboration between Government and Aboriginal Community Controlled Health Services.
2. Implement Housing and Infrastructure initiatives to improve Aboriginal (empowering communities through education and employment opportunities)
The options will be assessed against 3 criteria to ascertain their overall effectiveness:
· The ability of the scheme to improve the health status of Aboriginal and Torres Strait Islander people.
· The ability of the scheme to be sustainable in remote areas
· The ability of the scheme to be economically viable
Decision Making Matrix
| Criteria Option | The ability of the scheme to improve the health status of Aboriginal and Torres Strait Islander people. | The ability of the scheme to be sustainable in remote areas | The ability of the scheme to be economically viable |
| Proposal One Increase the collaboration between Government and Aboriginal Community Controlled Health Services. | Positives + It will be controlled by Aboriginals, so it is culturally sensitive + Aboriginals looking after Aboriginals + Aboriginals get education and work for health services + Controlled by government + Will have more attendance because of other Aboriginals who actually work there + Dialysis treatment in communities Negatives - Lack of understanding due to difference between cultures - Security of medications - Lack of facilities - Communities still will be in scarcity of doctors | Positives + Culturally sensitive due to other Aboriginals controlling + Government monitoring health care + Eliminate chronic disease + Will have more attendance because of other Aboriginals who actually work there + People will not be isolated due to living in the community Negatives - Lack of understanding due to difference between cultures - Security of medications - Lack of facilities - Communities still will be in scarcity of doctors - Cultures will be effected by new accommodations | Positives - Government monitoring health care - Free health care - More jobs for Indigenous people Negatives - Expensive monitoring - Cost of providing doctors, equipment, new buildings, etc. to rural areas - Cost of educating the Indigenous - Cost of going out to rural areas |
| Proposal Two Implement Housing and Infrastructure initiatives to improve Aboriginal (empowering communities through education and employment opportunities) | Positives + New or improved services + Improved living standards due to new houses + Improved nutrition, so health will be improved too Negatives - Can cause accidents due to lack of knowledge how to explore new services (fires, floods, etc.) - Will be expensive for Aboriginals to pay taxes and bills | Positives + Developing people (new knowledge, learning the world) + Collaboration of people + Sense of responsibility Negatives - Ongoing maintenance services - Will be expensive for Aboriginals to pay taxes and bills - Work out of communities - Not a traditional culture | Positives - Training people - Employment opportunities - Private income for those who organise Negatives - Expensive - Cost of going out to rural areas - Cost of providing doctors, equipment, new buildings, etc. to rural areas |
Evaluation of Proposals
Both proposals are to manage Type 2 Disease amongst Aboriginal and Torres Strait Islander people. Proposal One and Proposal Two have either negative or positive effectiveness in three criteria. The Proposal which will more successfully provide primary health care for Aboriginal and Torres Strait Islander people who are suffering from diabetes, will be recommended in this report.
Proposal One recommends to increase collaboration between Government and Aboriginal Community Controlled Health Services. Proposal One can improve the health status of Aboriginal and Torres Strait Islander people because it would be culturally sensitive, Aboriginals will control health care services in communities. Attendance to hospitals will improve because service will be provided by other Aboriginals who actually work there. A Dialysis treatment in the communities will be developed due to regular government support of health care services. There are some issues which will slow down effectiveness of the Proposal One; Indigenous and Non-Indigenous cultures are different, this issue can lead to lack of understanding between these two cultures, communities still will be in scarcity of doctors. Lack of facilities, government will not be able to provide all required equipment due to a lot of communities.
Proposal Two will empower communities through education and employment opportunities. The health status of Aboriginal and Torres Strait Islander people will be improved owing to new improved services. Living standards will also improve, nutrition would improve and therefore health of Aboriginals would improve. Housing and Infrastructure initiatives can cause accidents of flood or fire due to ignorance of implementation of new services such as electricity or water-supply. Also Aboriginals may not be able to pay taxes and bills for provided services.
Another important issue for proposals to become effective is the ability to be sustainable in remote areas.
Proposal One is Government monitoring health care services; it will eliminate chronic disease and will have more attendance due to Aboriginal controlling. It is very good opportunity for communities to improve health services. However lack of understanding will still exist, as well as a lack of facilities. New accommodations can be related to negative influence on Indigenous culture, but new accommodations still will improve health service.
Proposal Two will introduce collaboration and sense of responsibility to communities. People will have jobs, they will learn more about the world and about health lifestyle. Education and employment opportunities will lead to abilities to work out of the communities, it can cause deserted communities and loss of culture.
Both proposals are expensive and have costs of going to rural areas, educating Aboriginals, providing doctors, equipment and buildings. Proposal One will provide free health care and more jobs to Indigenous people. Also it is Government monitored, so, it is supported by Government funding. Proposal Two will train people and also will provide jobs.
Recommendations
Proposal One, increase the collaboration between Government and Aboriginal Community Controlled Health Services, will be more effective in managing chronic disease amongst Aboriginal and Torres Strait Islander people. It is Government monitored, reliable organisation. All strategies of the Proposal One will positively impact health care services. Indigenous culture will not suffer from implementation of new lifestyle due to actual collaboration between Indigenous and non-Indigenous health services. Aboriginals serving Aboriginals, attendance of health service will improve. Proposal One is recommended for its viable option to successfully provide primary health care for Aboriginal and Torres Strait Islander people who are suffering from diabetes.
Conclusion
Type 2 Diabetes is widely spread amongst Aboriginals a Torres Strait Islander people. It is a major contributor to indigenous mortality. The risk factors which cause chronic disease include those at the individual level, such as poor diet, physical activity, smoking and alcohol consumption, as well as factors affecting the entire community such as post-colonisation issues, low socioeconomic status and cultural beliefs. Australian Government contributes medical and social strategies to manage chronic disease amongst Aboriginals. A multifactorial approach was used to understand the high prevalence of disease. Recommendation of the Proposal One was made for prevention, including strategies aimed at the whole community while keeping their cultural beliefs.
8. Bibliography/Reference List
1. A healthdirect Australia health information service (2012). Viewed 23rd October 2012, http://www.healthinsite.gov.au/topics/diabetes
2. A healthdirect Australia health information service (2011). Viewed 22nd October 2012, http://www.healthinsite.gov.au/topics/Risk_Factors_for_Diabetes
3. AIHW (2012). Viewed 23rd October 2012, http://www.aihw.gov.au/diabetes/
4. Shukla, A. (2010). Viewed 30th October 2012, http://eview.anu.edu.au/cross-sections/vol6/pdf/ch05.pdf
5. AIHW (2012). Viewed 23rd October 2012, http://www.aihw.gov.au/diabetes/populations-of-interest/
6. UBM Medica Australia (2003). Viewed 16th October 2012, http://www.mydr.com.au/diabetes/diabetes-in-aboriginal-australians
7. Peter Azzopardi, Alex D Brown, Paul Zimmet, Rose E Fahy, Glynis A Dent, Martin J Kelly, Kira Kranzusch, Louise J Maple-Brown, Victor Nossar, Martin Silink, Ashim K Sinha, Monique L Stone and Sarah J Wren (2012). Viewed 16th October 2012, https://www.mja.com.au/journal/2012/197/1/type-2-diabetes-young-indigenous-australians-rural-and-remote-areas-diagnosis
8. T2DM Guideline Series (2012). Viewed 16th October 2012, http://www.rhef.com.au/programs/program-1/?program_id=384
9. Queensland Government (2012). Viewed 8th October 2012, http://www.qld.gov.au/disability/community/facts-terms/types/diabetes.html
10. Diabetes Australia (2012). Viewed 16th October 2012, http://www.diabetesvic.org.au/type-2-diabetes/aboriginal-and-torres-strait-islander
11. Queensland Government (2012). Viewed 8th October 2012, http://www.health.qld.gov.au/chronicdisease/documents/strat2005to15_full.pdf
12. The National Diabetes Service Scheme (2012). Viewed 30th October 2012, http://www.ndss.com.au/Australian-Diabetes-Map/Map/
13. Payne. S, (2012). Spinifex State College, Mount Isa. QLD

Appendix
http://www.ndss.com.au/Australian-Diabetes-Map/Map/
Figure 1. Diabetes Type 2 in Australia (2012)
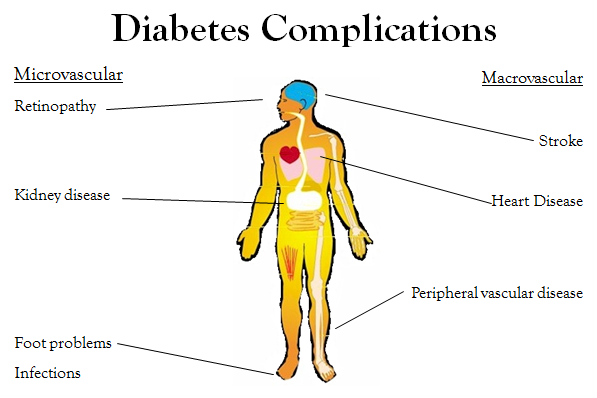
Figure 2. Diabetes Complications (PPT).
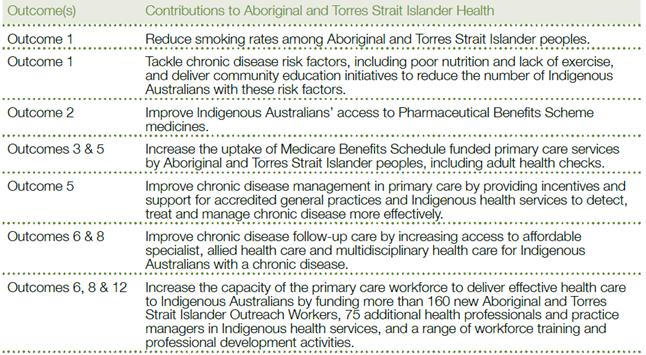 Figure 3. Australian Government Contribution to National Partnership Agreement on Closing the Gap in Indigenous Health Outcomes (Australian Government, 2012)
Figure 3. Australian Government Contribution to National Partnership Agreement on Closing the Gap in Indigenous Health Outcomes (Australian Government, 2012)
Дата добавления: 2015-10-29; просмотров: 215 | Нарушение авторских прав
| <== предыдущая страница | | | следующая страница ==> |
| Causes of Diabetes | | | By Associated Press, Published: June 21 |