§ 20% of all strokes
§ Caused by occlusion of deep penetrating cerebral arterioles
§ Small deep infarctions located in the deeper portion of the brain and brainstem. Lesions are deep in the brain and do not impair higher cortical function
§ Risk factors include hypertension (HTN) and diabetes mellitus (DM)
§ Cerebral lesions are small so they do not cause severe impairment or disability
§ Well recognized:
. Pure motor hemiparesis
. Pure sensory syndrome (impaired tactile discrimination, sensory ataxia)
. Dysarthria – clumsy hand syndrome (dysarthria owing to paresis of lip, tongue, and jaw musculature)
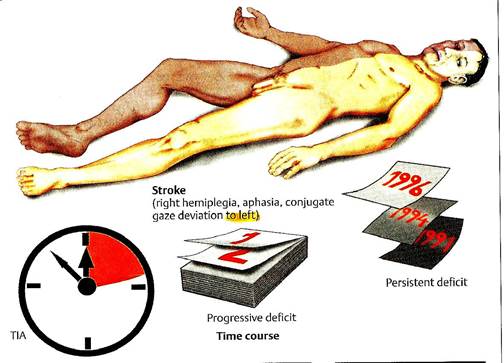
TRANSIENT ISCHEMIC ATTACKS (TIA)
© Are episodes of vascular insufficiency that cause temporary loss of brain function, with total recovery within 24 hours
© New definition: brief episodes of neurologic dysfunction caused by focal brain or retinal ischemia lasting < 1 hour and without evidence of acute infarction
© Most TIAs last for less than half an hour, with no residual signs at the time of clinical examination
© Most attacks follow lodgment of fibrin clots or detached atheromatous tissue at an arterial branch point with subsequent dissolution
A. Transient symptoms in the anterior circulation:
- Motor weakness (a heavy feeling) in an arm or leg; dysphagia
- Hemisensory deficit (a numb feeling)
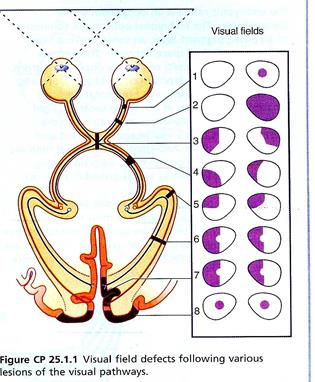
- Monocular blindness from occlusion of the central artery of the retina (amaurosis fugax)
B. Transient symptoms originating in the post circulation:
- Vertigo
- Diplopia
- Ataxia
- Amnesia
COMPUTED TOMOGRAPHY (CT)/MAGNETIC RESONANCE IMAGING (MRI) OF HEAD
* All patients with suspected stroke should have an emergency non-contrast enhanced CT scan or MRI to differentiate ischemic from hemorrhagic stroke and to identify tumor or mass effect (suggesting large stroke)
* Ischemic stroke is the most likely diagnosis when CT scan does not show hemorrhage, tumor, or focal infection, and the clinical findings do not suggest migraine, hypoglycemia, encephalitis, or subarachnoid hemorrhage
* MRI is more sensitive than CT scan for detecting brain infarction within the first 72 hours and for evaluating the posterior fossa (brainstem and cerebellum)
* CT can better differentiate hemorrhage from ischemia in acute lesions
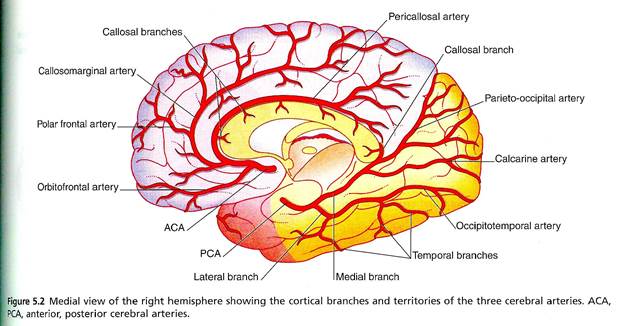
ANATOMY
4 Anterior cerebral artery (ACA) stroke affects contralateral lower limb
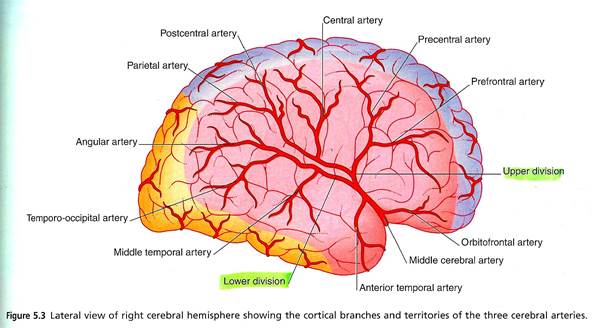
4 Middle cerebral artery (MCA)
. End branch infarcts of the MCA affect the contralateral upper limb and, if on the left, language function
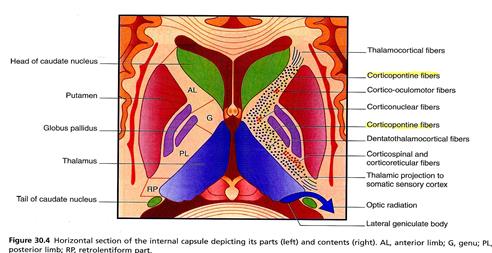
. More proximal infarcts affecting the distribution to the internal capsule cause full contralateral hemiplegia with drooping of the contralateral lower faces
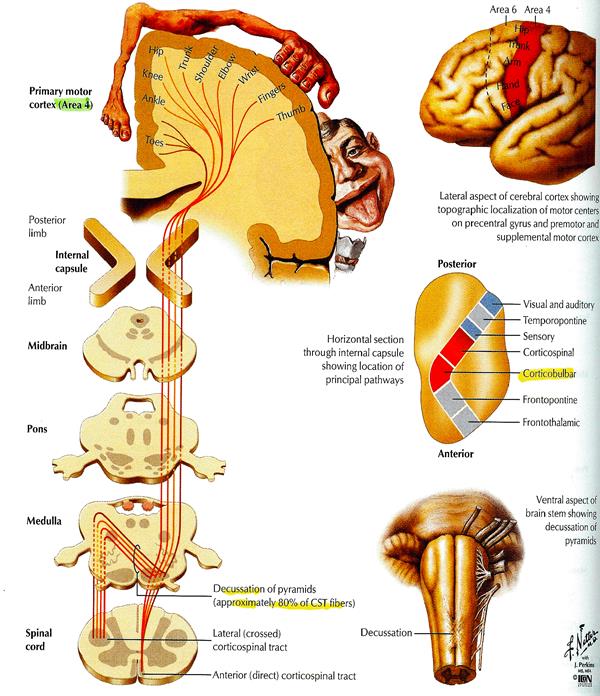
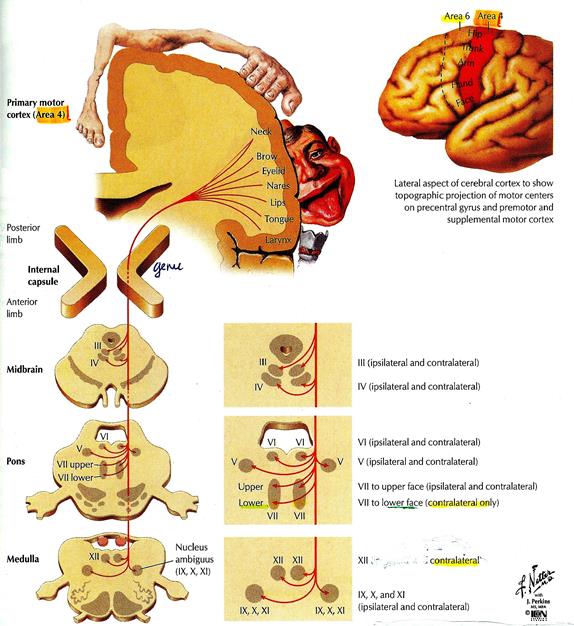
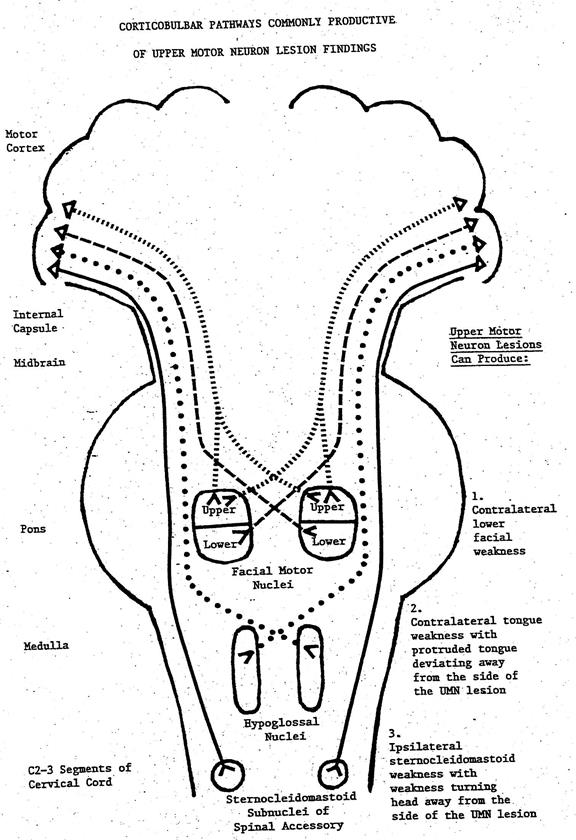
Ÿ Facial nerve
Ø The lower face receives contralateral projections of the corticobulbar tract (CBT) exclusively
Ÿ Hypoglossal nerve
Ø CBT projections to the hypoglossal nucleus are mainly contralateral
Ÿ Spinal accessory nerve
Ø CBT projections to spinal accessory nucleus are mainly ipsilateral
Дата добавления: 2015-10-30; просмотров: 114 | Нарушение авторских прав
| <== предыдущая страница | | | следующая страница ==> |
| GUIDELINES FOR PRIMARY PREVENTION OF STROKE | | | LANGUAGE AREAS |